
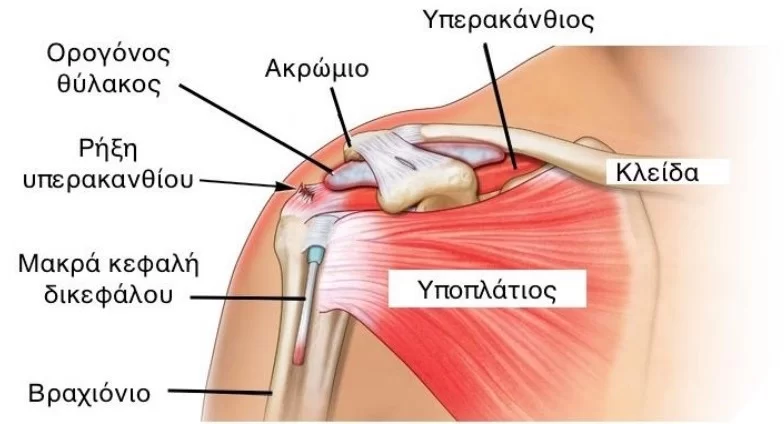
Traditionally, the term Impingement Syndrome has been used to describe compression of the soft tissues in the subacromial space (ie a space located below the acromion, in the shoulder).
This term has been around for about 50 years, first popularized in the 70s by Dr. Neer: was convinced that most rotator cuff tears he saw in clinical practice were caused by impact.
He then suggested surgery to “correct” such an impingement by removing some anatomical structures found in the shoulder to “make more room” and reduce tissue compression within the subacromial space.

Today, however, we have high-quality evidence showing that:
👉 This surgery is NOT better than exercise.
👉 Also recommending that the term “shoulder impingement” be abandoned.
We also know that:
✅ Compression in the subacromial space is common.
✅ Happens with daily tasks.
✅ It can occur in people with symptoms as well as in people without.
✅ reduced subacromial space is NOT associated with symptoms/pain or disability.
Shoulders can hurt for a variety of reasons (pain is complex!) and most of the time it’s not even possible to pinpoint a specific structure to explain the symptoms.
And the truth is, as long as a patient is experiencing non-traumatic shoulder pain that isn’t related to specific conditions like, say, frozen shoulder, then the treatment isn’t going to change much based on the label we put on it, but rather the person who we have before us.
A complete physical therapy protocol for the rehabilitation of impingement syndrome should, in addition to these therapeutic means, include mobilizations (Manual Therapy) of both the shoulder girdle and the thoracic spine of the Spine, the use of other therapeutic means, such as Kinesio Tape, and mainly therapeutic exercises aimed at retraining and restoring neuromuscular coordination and brachial rhythm.